Unstable Expansion: The Development of the Military Medical Evacuation Chain in Korea, 1948–1953†
Article information
Abstract
This research examines the expansion and characteristics of the Korean Army’s chain of medical evacuation in 1948–1953. The most important goal of the chain of medical evacuation was to conserve fighting strength, which cannot be achieved only by sending the sick and wounded to the rear for treatment. It was more important to maintain as many mission-capable wounded soldiers on the frontline. Therefore, triage for conserving strength was the priority in the evacuation process, and military doctors conducting triage played a significant role. Focusing on military doctors, this article studies the instability of the Korean Army’s medical evacuation chain.
Although Korea was liberated from Japanese colonial rule in August 1945, Korea had no army or army medical services. With the support of KMAG, the Korean Army was able to build a nationwide evacuation chain during the Korean War. However, the expansion of the medical evacuation chain resulted in instability. At the heart of the instability was manpower, rather than organization and transportation. Koreans had almost no experience with the military medical services before 1948, and during the Korean War, most doctors, who had been conscripted after the outbreak of the war, were not trained as military doctors. Therefore, the Korean Army had no other choice but to conduct medical evacuations using mobilized civilian doctors who were not sufficiently trained as military doctors. The escalating war revealed the problems of civilian doctors in military uniforms. Unlike the goal of the chain of medical evacuation, they easily evacuated patients and were reluctant to release patients to return to their duties. Korean Army doctors who were not sufficiently trained as military doctors struggled between the goals of military medical services and those of medical care. Consequently, the military doctors and the instability of the medical evacuation chain during the Korean War reflect the fundamental tension between war and medicine.
1. Introduction
“To put it simply, the improvement has been extremely marked, considering the fact that less than three years ago the medical service was extremely meager. Today, the ROK [Republic of Korea] Army Medical Service probably exceeds that of any other Asiatic military group and begins to compare favorably with our medical service as is existed perhaps early in this century. …… I feel that in no equal time period have we ourselves equalled the improvement made in the ROK Army since 1 July 1950.”1)
On February 24, 1953, George E. Armstrong, the surgeon general of the United States (US) Army, reported to the secretary of the army regarding the astonishing development of the Korean military medical service after visiting Korea. According to him, the Korean military medical service, which had been meager until July 1950, ranked the highest in Asia through the support of the US military. This support included the establishment of an American-style military medical system after the outbreak of the Korean War. This evaluation was due to the development of a military medical support system suitable for the expansion of the Korean Army, which grew from eight divisions at the start of the war to 18 around the time of the armistice. This was a remarkable change. However, if one closely observes the Korean Army’s chain of medical evacuation at the time, Armstrong’s evaluation avoids discussing any instability.
Conducting military medical evacuations was founded in Egypt around 1200 B.C., but it was conducted systematically only after the 18th century in Europe, and it was after the American Civil War (1861–1865) that evacuating mass casualties by trains became vital to war (Haller, 2011: 1-55). The reason why military medical evacuation became vital to war was that it served to avoid the permanent loss of fighting strength and to maintain the morale of soldiers. Therefore, the most important goal of the chain of medical evacuation, which is the entire group of successive agencies and installations involved in evacuations, is to conserve fighting strength (Medical Field Service School, 1950: 34; The Military Service Publishing Company, 1945: 347). The conservation of fighting strength cannot be achieved only by sending the sick and wounded to the rear and for treatment. It is more important to maintain as many mission-capable wounded soldiers on the frontline. Evacuations of patients not only impose an unnecessary burden on the military for transportation, treatment, and replacement but also weaken the strength of combat units. Therefore, triage for conserving strength is “a most important function of every medical agency,” and military doctors play a significant role in the medical evacuation (Medical Field Service School, 1950: 35). Notably, most Korean Army doctors were rapidly mobilized during the war. In this context, if we focus on medical evacuations and the military doctors who conducted them, we can unearth cracks in Armstrong’s evaluation. This article focuses on medical evacuation as a procedure to conserve fighting strength.
Although research on the Korean War and medicine has recently been conducted, research on the Korean Army, one of the largest groups providing medical care during the Korean War, remains on the fringes. Understandably, the medical evacuations of the Korean Army have not received much attention. This have been briefly mentioned in previous studies. In The Medics War, Cowdrey briefly discusses the development of the Korean Army medical service through US military materials, while the ROK Armed Forces Medical Command describes this development based on the Korean Army’s materials (Cowdrey, 1990; Armed Forces Medical Command, 2004). Considering the lack of material related to the Korean Army’s medical service during the Korean War and the strong influence of the US advisory group, it was necessary to use both Korean and US documents; JEON Wooyong’s study is significant because both types of documents are used (JEON, 2011). Despite the lack of evidence, due to the nature of popular publications, JEON’s investigation is a pioneering study of the Korean military medical service. This study outlines the development of the chain of medical evacuation from the perspectives of quantitative growth and qualitative problems, including problems regarding doctors’ abilities and shortages. However, because JEON’s study did not focus on medical evacuation, it did not analyze the process thereof nor the characteristics of the Korean military doctors. Based on previous studies, this study analyzes the process of the medical evacuation, the characteristics of military doctors, and uncovers the instability of the Korean Army’s medical evacuation chain.
This study, which deals with the development and instability of the Korean Army’s chain of medical evacuation, seeks to utilize two approaches. First, it focuses on the role of the US Military Advisory Group to the Republic of Korea (KMAG). Following the end of World War II, the US began providing military aid to capitalist countries in Europe, the Middle East, and Asia to block Soviet expansion. The US dispatched military advisory groups to foster militaries and to facilitate the execution of military aid in the recipient countries. The first advisory group to Asian countries was established in the Republic of Korea in July 1949.2) KMAG designed the Korean Army as well as the military medical service. Therefore, it is necessary to examine KMAG’s activities and the difficulties they encountered by using the materials they produced.
Second, this study concentrates on Korean military doctors. The chain of medical evacuation not only moves wounded soldiers to the rear, but also prevents evacuations to conserve fighting strength. In this respect, military medical evacuations often conflict with medical practices that seek better treatment. Therefore, the military must train doctors to perform triages according to military logic. However, Koreans had almost no experience with the military medical services before 1948. Additionally, the war broke out less than one year after the establishment of the Medical Field Service School (MFSS). In conclusion, to the Korean Army, there was no other choice but to conduct medical evacuations using mobilized civilian doctors. The chain, operated by civilian doctors who lacked an understanding of military medical services, conflicted with the goal of conserving fighting strength. This demonstrates the nature of military medical services and the fundamental tension between war and medicine.
2. The expansion of the Korean Army’s chain of medical evacuation
1) The embryonic state of the army medical services before the Korean War
Korea was liberated from Japanese colonial rule in August 1945 but had no army or army medical department.3) All the necessary tangible and intangible elements had to be prepared to build the chain of medical evacuation, which was essential for the army’s medical services. The first, in the chain, was organization and transportation. Medical units and installations had to be organized from the frontline combat units to the rear army hospitals and connected by adequate transportation. Second, competent military medical personnel were required for each echelon in the chain. Treatment capabilities, including first-aid and patient triage, that could determine who should be transported and returned, needed to be developed.
Medical organizations began to develop before and after the establishment of the ROK Armed Forces in August 1948. In May 1948, the 1st Medical Battalion and Army Hospital were established to provide medical support, supplies, and training (Chief of medical section, 1956: 124). Subsequently, by July 1949, four additional army hospitals were activated. Meanwhile, the Korean Army faced difficulties in drafting and training military medical personnel. Essentially, Korean doctors who could become military doctors were few (JEON, 2011: 246). In 1947, there were 2,317 western-style doctors in South Korea; this is a very small number compared to the country’s population of approximately 20 million.4) Moreover, Koreans had almost no foundation in military medicine. It seems that the only person who had mastered the military medical system for a long time was SHIN Hakjin, who served in the Manchurian Army for 10 years and was the commander of a military hospital (Committee to publish SHIN Hakjin’s collection of works, 1971: chronological table; CHOI, 2015: 235; Health Newspaper Publishing Company, 1991: 112-118). At the same time, there was no military medical school within the first eight Korean Army schools (Sawyer, 1988: 79). Korean military medical personnel were trained in US military medical units and the Korean Military Academy.5) In addition, there were no manuals for them. Translated books were used for training by the 1st Medical Battalion (Chief of medical section, 1956: 124).
Medical personnel training improved in July 1949 with the establishment of KMAG. Education for military medical personnel began through regular courses, which were made possible by the MFSS, established in August 1949, with the support of KMAG.6) Accordingly, the training of medical evacuation was conducted in the regimental medical detachments.7) In addition, through a series of suppression operations from October 1949 to 1950, the army began to accumulate medical evacuation experience (ROK Army Headquarters, 1959: 130).
An important change in army medical services occurred in April 1950. As each army brigade was promoted to a division, the medical organization expanded. This was modeled after the US Army. The Korean Army introduced a chain of medical evacuation at the division level, which consisted of a regimental medical company and a divisional medical battalion (YUN, 1951: 231-232). In particular, the regimental medical company was the same as that of the US Army, which was introduced to strengthen regimental medical support after World War II (Cowdrey, 1990: 74; Darnall, 1949: 191-192). In April 1950, KMAG dispatched 33 officers, including medical officers, to the units of the US 8th Army in Japan to observe the administration, operation, and training methods of the US Army (Sawyer, 1988: 89). The purpose was to make the Korean Army understand the US-style Army.8) From April to June 1950, they closely observed and reported on the medical organization of the 1st and 2nd echelons.9)
However, the Korean Army’s pre-war development was limited. First, the Korean Army had no military medical foundation, regarding quantity or quality. Due to the lack of medical personnel in Korea, they faced drafting problems. Immediately before the war, there were only 183 medical doctors and 110 nursing officers in the army.10) This was inadequate for an army of approximately 95,000 soldiers in eight infantry divisions and 22 regiments. Making medical personnel understand military medical service was another problem. In January 1950, the advisory group’s Semi-Annual Report stated that military medical personnel training had not reached a satisfactory level.11) Korean military doctors used ineffective old Japanese methods and lacked knowledge of modern techniques and therapies. KMAG evaluated the effectiveness of the Korean military doctors by comparing them to the US military standards and found they met approximately 50% of these standards. Further, private soldiers met 25–30%, hospitals met 40–50%, and regimental medical detachments met 35% of US military standards. Koreans with no foundation in military medical services required considerable time. In addition, despite the plans made in April, the activations of the medical battalion and the regimental medical company were not completed.
However, difficulties in army medical services were not solely due to Koreans. The US military had failed to show an active interest in the Korean army medical service. The number of KMAG medical officers was few to care for Korean army.12) The formation of KMAG illustrates this well. Until June 1950, KMAG’s medical section consisted of only three officers, one nurse, and five soldiers.13) Compared to other sections, such as signal (eight officers, 36 enlisted men), ordnance (O-7, E-20), engineer (O-12, E-17), and quartermaster (O-7, E-8), this was a small number. In addition, the KMAG medical section was in charge of two functions: consulting the Korean Army and running a dispensary for KMAG’s staff. This was due to a shortage of military doctors in the US Army Medical Department (Cowdrey, 1990: 28-35). Therefore, just before the war, the Korean Army’s medical services were at a basic level, both regarding organization and manpower. As Armstrong evaluated, the state of the Korean military medical services before June 25, 1950, was “embryonic.”14)
2) The expansion of the chain of medical evacuation during the Korean War
In the early stages of the war, the Korean Army’s medical services were in chaos. As previously mentioned, not all aspects of quality and quantity met the standards for war. On June 25, Lieutenant YOO Inyoung, a surgeon of the 1st Battalion, 1st Regiment, 7th Division on the Western Front, was on vacation in Seoul. At approximately 12:00 noon, he heard the broadcast announcing a command to return, and he returned to the regiment in civilian clothes. When he arrived, the regiment was empty, and all the soldiers of the regiment were on the battlefront. He moved to the battlefront using a three-quarter ton truck. On the move, he panicked when he saw the wounded along the roadside. Lieutenant YOO did not have any medical equipment; hence, he collected patients and evacuated them to the division. However, as the number of patients was too large for this division, he evacuated the patients to Seoul National University Hospital (Armed Forces Medical Academy, 2004: 22).
This case shows that the forward chain of medical evacuation from the battalion to the division fell into chaos on the first day of the Korean War. Patient collection, sorting, and hospitalization were not performed appropriately. On July 7, 1950, the 3rd, 5th, 7th, and 9th divisions of the Korean Army activated divisional medical battalions, despite their inadequate conditions.15) Unlike the Western Front, which quickly collapsed in the immediate aftermath of the war, medical services in the mountainous Central and Eastern Fronts, which succeeded in delaying the enemy, operated better (Armed Forces Medical Academy, 2004: 23-24). The South Korean army did respond to the war. The army dissolved the MFSS on July 9 and activated three surgical teams with MFSS personnel and equipment (ROK Army Headquarters, 1959: 131; PARK, 2004: 82).
Even if the evacuations on the Eastern Front proceeded smoothly, a large number of the wounded were evacuated to the rear. This rapidly paralyzed the rear army hospitals. On the afternoon of June 25, 1950, patients began to enter the 1st Army Hospital (MOON, 2007: 84). Just before the outbreak of the war, the Korean Army Hospital had capacity for 2,250 patients; however, in the first three days of the war, 3,200 patients were evacuated. Two to three days after the start of the war, the battle lines were pushed back, and withdrawal operations began. Army hospitals with a large number of patients were forced to withdraw by train (Armed Forces Medical Academy, 2004: 10-11; ROK Army Headquarters, 1959: 131). The withdrawal of the army hospitals made the chain of medical evacuation even more difficult. The army hospitals faced two challenges: moving with critically ill patients, and constant movement owing to the rapid southward movement of the frontline. The rear became the front within a few days and the location of the army hospitals changed occasionally (ROK Army Headquarters, 1959: 131). No rear army hospitals could stably accommodate wounded from the front.
Under these circumstances, running an army hospital was difficult. The scene PARK Yongha encountered at a branch of the Capital Army Hospital, which had moved to Suwon, was chaotic. He stated, “Because of the entwined ambulances transporting wounded soldiers and vehicles, the main gate of the army hospital reminded me of a roundabout in a downtown area with paralyzed traffic lights.” Many patients were evacuated to army hospitals that were on the move. Emergency surgeries were performed at hospitals; however doctors and equipment were limited, and there were too many injured patients requiring surgery and treatment. Additionally, the army doctors did not have proper manuals.16) Classifying the wounded was difficult and required a considerable amount of time to determine the order of the emergency operations. Many soldiers died while waiting for their turn. Thus, to respond quicker, Park notes, “Sometimes, if the bullet that was stuck in the body didn’t injure any vital organs, I would just disinfect it and evacuate the wounded to the rear.” (KIM, 2003: 101-105)
From August 1950, the Korean Army’s chain of medical evacuation was expanded and reorganized. On August 19, H.J. Witte, KMAG surgeon advisor, established a plan called “Medical installations required for Ten Korean Army Division.”17) This plan intended to provide medical support to the newly expanded army from August. Therefore, it was necessary to construct an adequate chain of medical evacuation. The plan had ten divisions, each with one medical battalion and each regiment with a regimental medical detachment, to facilitate the evacuation of the combat units, ten army hospitals, and five surgical teams. As a result, divisional medical battalion, two surgical teams, and seven army hospitals were activated until the end of 1950. In addition, the establishment of transportation units was planned which included the activation of an ambulance battalion controlled by the surgeon general of the Korean Army. The ambulance battalion divided the 60 ambulances into ten subgroups and each group planned to assist in the evacuation from the division to army hospitals. In addition, the training of military medical personnel, which had been suspended, was considered, and the MFSS was re-established on November 7, 1950.
In addition to the expansion plan, conscription and activation of hospital train units eased the confusion during the early stage of the war. After July 1950, the Korean military conducted de facto conscription. Although conscription by the Korean military was not legislated, the military drafted young men through violent methods. In addition, many young men, including doctors, volunteered for the military out of fear of being branded a communist (YOON, 2019: 124-139). In this atmosphere, whether voluntary or involuntary, many Korean doctors joined the army. This de facto conscription alleviated the army’s shortage of military doctors. The expansion of the army's medical system could only be sustained by this de facto conscription.
Important developments regarding transportation were made between December 1950 and January 1951. Three hospital train units that enabled mass transportation of the wounded, were established (YUN, 1951: 232-233). Based on the expansion described above, unlike earlier in the war, the Korean Army was able to evacuate the wounded without confusion, even during the large-scale retreat that began in December 1950 (Armed Forces Medical Command, 2004: 28-29).
The series of reorganization processes for the army’s chain of medical evacuations ended in March 1951. The final task of the expansion was to switch the surgical team to a mobile army surgical hospital (MASH) on March 31, 1951 (Armed Forces Medical Command, 2004: 26). The introduction of the MASH units symbolized the development of the Korean Army’s chain of medical evacuation in the American’s style. Given that the first US MASH units were activated in Japan in July 1950, the introduction of the MASH units to the Korean Army showed that the latest US-style military medical service was applied in the wake of the Korean War (Cowdrey, 1990: 69-70). After March 1951, the Korean Army ran the chain of medical evacuation from battalions to divisions, MASH units, and army hospitals. The chain was positioned as the basic framework of the Korean military medical system not only during the war but also after the armistice. In December 1952, the US Army Field Forces Observation Team evaluated the Korean Army’s Chain of medical evacuation as follows: “The evacuation of the Republic of Korea Army personnel is a separate system parallel to the US system.”18)
3. Civilian doctors in military uniforms
Based on the reorganization and expansion, the Korean Army operated a nationwide chain of medical evacuations, with the goal of conserving fighting strength. The army’s medical units and installations tried to maintain mission-capable soldiers on the frontline by elaborately sorting the wounded to determine who could still fight. The sorting process began at the battalion aid station. In general, those who were wounded during fighting received first aid from medics in the combat area, and then the ambulatory wounded moved to a battalion aid station or ambulance pick-up point. The non-ambulatory wounded were carried by litter-bearers (ROK Army Headquarters, 1953).19) However, except for the seriously wounded, who were to be directly evacuated to the MASH, the wounded who arrived at the aid station had to go through a difficult process to be evacuated to the army hospital. They had to go through the regimental collecting station and the divisional clearing station. This was because the goal of the medical evacuation was more focused on conserving fighting strength than providing treatment in the rear. Although written one year after the armistice, the writing of Lieutenant HAN Dongse, a military doctor at the Capital Army Hospital, illustrates this well. He classified patients into two categories: those to be returned to their unit and those to be discharged from the army (HAN, 1954). This illustrates the army’s view on wounded soldiers. From HAN Dongse’s perspective, “The patients in the division must be decided whether to return to their unit or evacuate to the rear within a week. Eighty percent of them have to be returned and only the remaining 20% will be evacuated” (HAN, 1954). He emphasized the goal of conserving fighting strength within the division.
This was possible through triage. From battalion aid stations to army hospitals, each echelon’s role was to triage to conserve fighting strength, and constantly filter the wounded. This was presented as ideal according to the Korean Army’s field manual (ROK Army Headquarters, 1953: 182-191). The field manual for the Korean Regimental Medical Company, published on March 20, 1953, emphasized its role as a filter: “Constant efforts must be made to avoid unnecessary evacuations. Patients with minor injuries and illnesses should be returned to their unit after treatment.” Similar work was carried out in the regimental collecting station. “The regimental collecting station is operated as a buffer against excessive troop depletion. Injured individuals who are expected to return to their unit, within a reasonable period, should be placed in the collecting station until they return to their unit” (ROK Army Headquarters, 1953: 187). According to the manual, the collecting station was a filter that prevented the depletion of troops, thereby demonstrating the primary goal of the station. After passing through the regimental filter, the wounded were evacuated to the division with an emergency treatment tag. Although the medical installation of the Korean Army division’s specific mission is not clear owing to a lack of records, considering HAN Dongse’s mention, it would have had a similar purpose.
The army hospitals were the next destination for the wounded evacuated from a divisional area. Evacuations from these divisional areas to army hospitals were generally conducted using hospital trains and ambulances (Armed Forces Medical Command, 2004: 30). Just as the medical installations in the division area aimed to conserve fighting strength, the rear army hospitals had to return the wounded to duty as soon as possible. HAN believed that patients arriving at army hospitals had to return to duty rather than be discharged from the army and that the number of patients admitted to hospitals should be reduced (HAN, 1954). Accordingly, the army attempted to encourage the hospitalized wounded to return to duty. For this reason, the army held send-off parties for returning soldiers and conducted military spirit education such as “Homeland’s Expectations and Our Resolution” and “Society and Our Path Seen from a Hospital Window” in army hospitals for those who had to return to their unit (Troop Information and Education General’s Office, 1952: 62-63).20) Thus, to conserve fighting strength, unnecessary evacuation of the wounded from the front had to be prevented as much as possible, and the wounded in army hospitals had to return to duty as soon as possible.
Therefore, from the battalion aid station to the army hospital, the chain of evacuation aimed to act as a filter to prevent the depletion of fighting strength. However, this did not ideally materialize. Despite the expansion of medical organizations, transportation and manpower problems persisted. Transportation problems persisted within the division area. Evacuation from the combat area, which commonly depended on manpower, was dangerous for litter-bearers and the wounded. The lack of equipment intensified this issue. Serious shortages in litters and ambulances were reported by the end of 1951.21) This shortage continued until the armistice.22) Additionally, on the Central and Eastern Front, extensive mountainous terrains caused tremendous medical problems.23) Owing to the poor road conditions, it was difficult for ambulances to enter the mountainous areas.24) However, evacuation problems in this area were alleviated considerably in early 1953 when the army finished building military roads and cable lines in the most rugged mountainous areas.25) In addition, trolleys and cable lines, which are means of transportation suitable for mountainous terrain, were introduced into the MFSS training course in March 1953.26)
Manpower was a more significant issue. Triage, conducted by military doctors, was the most important process to conserve strength. One case illustrates the role and importance of military doctors in the triage process. Here, a military doctor at the 5th Army Hospital discharged Kim Jeom-Seok, who broke his back and could not fight, from the hospital and assigned him to the 2nd recruit training center as an assistant instructor rather than remove him from the army. To make the most of the wounded, from the army’s perspective, the military doctor gave him the maximum amount of tasks he could perform. Kim could not refuse the order and, as a result, suffered from back pain for the remainder of his life.
The military doctor’s behavior towards Kim was exemplary and in line with the goals of the military medical services. The behavior of military doctors differed from that of civilian doctors. The military doctor regarded Kim as a wounded soldier rather than just a patient and returned him to duty without complete treatment. Nevertheless, Kim was luckier than the others. According to those who participated in the war, despite their injuries, army hospitals remained inaccessible (JUNG, KIM, SO, 2014: 38; 143-145; 166). According to the soldiers’ recollections, the army tried to return the wounded veterans to their units. Although their injuries were substantial, they were not evacuated to an army hospital and had to return to duty before recovering. From their memories, we can understand the hardship and dissatisfaction experienced by the wounded. The military doctor’s sorting criteria to determine evacuation were too high, according to the injured.
The military doctors prevented the wounded soldiers from being evacuated and prioritized returning them to duty after reaching a certain level of recovery by performing triage. This kind of military-oriented logic and attitude, which differed from that of civilian doctors, was possible through military training. The MFSS was responsible for training such exemplary military doctors. From KMAG’s perspective, “civilian medical educational facilities” alone could not complete the military medical personnel, and “The fundamental requirement for such military-medical education was obvious in consideration of the primary supportive service of the medical program to an army.”27) In the MFSS, medical personnel could be completed as military medical personnel by developing military-specific prevention, curing, and sorting capabilities.
However, the number of military doctors trained through the MFSS was low for most of the Korean War. After the outbreak of the war, the Korean Army needed many doctors because of the expansion of the army and the rapid increase in the number of the wounded. Under the influence of de facto conscription, the army appointed civilian doctors as military doctors. In this system, civilian doctors were given ranks immediately on the spot such as army hospitals and sent to the front line (KIM, 2003: 120). They were called “on-the-spot commissioned officers.” Some hospitals were converted into military hospitals with all their equipment and personnel. For example, in December 1950, the 2nd Seoul National University Hospital was converted into the 36th Army Hospital, which was upgraded to a Capital Army Hospital in October 1953. Subsequently, all the hospital staff members belonged to the military. In addition, a fourth-year student at Seoul National University’s Medical School was appointed as a second lieutenant and immediately placed on the frontline (KIM, 1979: 147-148; 150-151). Military training of the on-the-spot officers was rarely performed. The experience of MOON Taejoon, who graduated from medical school in May 1950 and was assigned as a battalion surgeon on the frontline in January 1951, demonstrates the level of training given to military doctors at that time. He stated, “The basic training I received in Busan for two weeks was limited to salutes and knowledge of the military organization, which was not useful for the actual evacuation of patients in the combat area;” therefore, he had to “take responsibility for the battalion with the help of the first sergeant” (MOON, 1999: 51). In this respect, on-the-spot military doctors were more similar to civilian doctors in military uniforms than to military medical personnel. Neither were they fully civilian doctors nor were they sufficiently trained as military doctors.
On-the-spot military doctors accounted for more than 80% of the medical evacuation chain. Of the 871 Korean Army doctors at the end of 1951, despite including all 183 doctors who were commissioned before the war, on-the-spot officers accounted for at least 79%. In addition, re-education was almost non-existent. At the end of 1951, KMAG complained about the serious shortage of doctors in the Korean Army. According to KMAG’s claims, there were only 871 military doctors, although the present table of organizations should have 993. They have also stated that “In order to furnish medical care for the expansion of ROKA to present proposed limits, it is necessary to increase the number of doctors from the present 871 to 1315.”28) Owing to a lack of manpower, it was difficult to reeducate military doctors in the rear area. Even though the MFSS had a basic officer course after May 1951, there was only one session with a three-week short course for 50 doctors in 1951.29)
From 1950 to 1952, the MFSS was an institution for “medical enlisted men” and “medical technicians.” By December 28, 1952, the training of 4,869 enlisted men and 1,054 technicians had been completed; however, only 128 military doctors, 180 medical service officers, and 11 nursing officers had been trained.30) Although an eight-week Medical Department Basic Officers Course was introduced on January 28, 1952, only one session with 50 doctors was conducted in 1952.31) Although the MFSS trained approximately 800 civilian doctors between January and June 1953,32) this was a four-week short-term reserve course based on the medical personnel draft issued by the Korean government.33) These newly trained doctors could be appointed as military or public dispensary doctors. However, in 1953, at least 25% of the 3,700 western-style doctors in South Korea were military doctors, and due to concerns about a shortage of civilian doctors,34) only some of the newly trained doctors became military doctors.35) Therefore, although new civilian doctors were trained at the MFSS in 1953, on-the-spot officers were still the majority of the chain of medical evacuation, both in numbers and in experience. In short, for most of the war, the army utilized on-the-spot officers who were not sufficiently trained as military doctors to maintain the chain of medical evacuation.
Although on-the-spot commissioned officers did not receive sufficient training as military doctors, they were indispensable. Not only did they fill the shortage of military doctors but they also competed with the existing military medical officers commissioned before the war regarding their abilities. Existing military doctors seemed incompetent in the eyes of KMAG and the Korean Army. For example, Nursing Officer CHO Gwirye identified that pre-war military doctors lacked ability but had high self-esteem. Veteran’s ability was an important difference compared to the US military doctors. During the Korean War, the US military faced problems with the experience of military doctors. When the war broke out, there was a shortage of military doctors and the US military had to utilize civilian doctors with no military experience. However, the US military had qualified veterans who had experienced World War II and could team up with newly trained doctors (Cowdrey, 1990: 139-141). However, in the Korean Army, not only were on-the-spot military doctors occupying most of the chain of evacuation, but there were also no veterans to trust or rely on. Existing military personnel relied on on-the-spot military doctors. The death of an on-the-spot military doctor was a serious blow to an army hospital. CHO Gwirye spoke about the need for them: “It is difficult to image how we would have overcome the difficult situation at that time if there had been no temporary system of on-the-spot commissioned officers. The necessity makes a system” (MOON, 2007: 105; 109; 117-118).
However, these doctors had to become military medical personnel. From CHO Gwirye’s description, we can see the military’s suspicious view toward on-the-spot officers: “Some nursing officers who entered military through on-the-spot cases lacked military spirit” (MOON, 2007: 212). Although this was a criticism of nursing officers in romantic relationships, we can see the military’s negative attitude toward on-the-spot officers’ insufficient military spirit.
The instability of on-the-spot doctors appeared as the war escalated again. From the end of September 1952, when the combat for high ground intensified, the chain of medical evacuation began to show signs of instability.36) Fierce fighting between the end of September and November led to a sharp increase in the number of evacuated patients [Table 1]. The number of hospitalized patients, which averaged approximately 6,000, doubled in October. Since then, the number of hospitalized patients decreased, but the number of discharged patients, which averaged approximately 5,600, except in July, dropped to an average of 4,700 from October onwards. This indicates that although the number of hospitalized patients increased, they were not discharged.
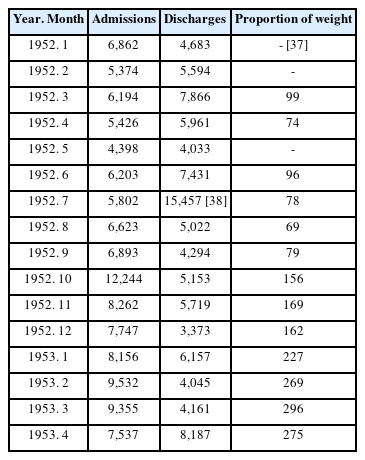
Monthly admissions, discharges, and deaths of the Korean Army hospitals, 1952–1953
The escalation of the war made it clear that the Korean Army medical installations were reluctant to release patients to return to duty.37) It was necessary for the wounded to return to duty to conserve fighting strength, but the military doctors concentrated on treating the wounded who had been evacuated after a fierce battle. The Korean military doctors acted as if they believed that the wounded should be treated for longer than the army thought. On November 25, the KMAG medical section requested an additional assignment of two medical corps officers to advise the Korean army hospital commanders on the discharge of patients. The problem persisted until December:38) “Continued stress is being made for the discharge of patients from the ROK Army hospitals and convalescent centers.”39) In December, the KMAG medical section and the Surgeon General’s Office of the Korean army held a series of meetings to resolve such issues and planned to increase the rate of patient release after investigating the army hospitals.
An option that KMAG could consider was to directly dispatch an adviser to control the evacuation. However, the number of personnel in the KMAG medical section was limited.40) Although the number of medical advisors increased in 1952, it was difficult to directly control the nationwide Korean army’s medical installations using only 16 officers. The medical field was a particularly difficult area for KMAG. The last paragraph of the May 1952 KMAG Command Report illustrates this situation well: “The Republic of Korea is currently receiving aid from the United States on the basis of a 250,000man army, and that figure is now exceeded by nearly 100,000. As for US personnel, qualified artillery and medical advisors are urgently needed.”41) Given the ongoing program to strengthen the Korean Army artillery at the time, the seriousness of the lack of medical advisors was understandable.
The problem in the chain of evacuation reappeared when the fight for high ground reached its peak before the armistice.42) <Table 2> shows the hospitalizations of the Korean Army 2nd Corps MASH and Clearing Company, which were in charge of the steep mountainous area. As highland warfare intensified, the capacity of each medical installation exceeded 812%, 418%, and 928% in May.

The Korean Army ⅡCorps Hospitalizations, 1953. 2–1953. 7
The KMAG medical section noticed a problem in the medical evacuation chain.
“During the month of May it was brought to the attention of the Medical Advisory Group that minor illnesses in ROK Army Combat Divisions were being air evacuated out of divisions, thru MASH’s and taken to and treated in Army type Hospitals. Typical type cases evacuated were otitis media, contusions, gastritis, and miscellaneous minor complaints, normally treated on a duty status by similar American units.”44)
In the Korean Army, minor cases who were not allowed to evacuated in the US Army were evacuated by air. In other words, the Korean Army doctors conducted a different sorting process than that of the US Army.
The issue of air evacuation was emphasized; however, judging from the measures taken, it was not simply an air evacuation problem. The medical section of KMAG together with the Korean Army Surgeon General’s Office developed measures focusing on the triage in the evacuation process: “An Army wide policy was issued to Korean Medical installations defining cases which should be evacuated, depending upon severity of the disease or injury, type treatment, and expected length of hospitalization.”45) This was a measure to intervene deeply in the triage of Korean Army doctors. KMAG evaluated that these measures reduced not only the number of evacuations but also the burden on army hospitals and conserved the division’s fighting strength. However, it was difficult to solve evacuation problems simply by distributing the triage guidelines. The forward medical installations were in poor condition for treatment owing to a lack of equipment and beds. More importantly, triage involved subjectivity that relied on the judgment of military doctors, and the identity of the military doctors were not clearly distinguished from those of civilian doctors. As a result, a large number of the wounded were evacuated to the rear. As shown in <Table 3>, even after May, the evacuation figures differed from KMAG’s evaluation.

The evacuation figures from the Korean Army ⅡCorps to the 36 Army Hospital by transportation type
The Korean Army’s chain of medical evacuation had continuity throughout the Korean War, as it consisted of civilian doctors in military uniforms. Amid the expansion of the chain, the military doctors who conducted the triage, which were at the core of the evacuation, did not appear to be loyal to military-oriented logic. In 1954, one year after the establishment of triage guidelines and the armistice, HAN Dongse’s dissatisfaction indicated that the situation continued after the war (HAN, 1954). He points out that the number of soldiers discharged from the army increased rapidly after the armistice. In his view, evacuation and discharge were something that the military had to prevent as much as possible because it led to a drop in the morale of the army. He stated: “Unlike civilians, who wait to hear that they are not ill, soldiers want to hear that they are ill.” This shows the recognition that there is a difference between military and civilian patients, similar to the difference between military and civilian doctors. While criticizing the evacuation and discharge from the army in this manner, Han emphasized that the key to solving this problem was military doctors: “We, Korean military medical officers, are in a position to prevent this.” In addition, he presented the spirit of military doctors as the final solution by stating, “Military doctors should treat patients with conscience and pride [of military doctors], thereby reducing the number of hospitalized patients and, furthermore, reducing the number of discharges from the army at the hospitals.”
After the armistice, as the MFSS expanded its training programs such as the Medical Officer’s Advanced Course, and the Officer’s Refresher Course, the problem of the on-the-spot officers seemed to be gradually eased. However, the instability of the medical evacuation chain did not disappear. In November 1954, the Korean army expanded to approximately 660,000. To support this expansion, the chain of medical evacuation also expanded, and the army needed more military doctors than in wartime. The problem was how to sustain this huge system.
The army, which had sustained the expanded medical system through de facto conscription during the war, maintained the expanded medical system by not allowing military doctors to be discharged. In 1955, while long-serving soldiers were allowed to be discharged, military doctors were not included.46) Because the Army needed approximately 1,800 military doctors, more than the 993 needed in 1951,47) and the veterans who experienced the war were the core of the army’s medical system. Since 1956, as if controlling the water level of river through dam, the army tried to maintain the medical system by gradually allowing long-serving military doctors to be discharged. In July 1956, the army allowed 110 military doctors who served more than five years to be discharged, 39 in May 1957.48)
However, given that a petition for discharge was presented by long-serving military doctors less than two weeks after the first discharge, the number of long-serving military doctors who wanted to be discharged exceeded the discharge allowance considered by the army.49) They were not satisfied with the poor life in the army. The army’s scale of 660,000 personnel was excessively large compared with the size of South Korea’s economy, and the army could not afford to maintain the medical system without conscription and compulsion. Some military doctors maintained their livelihoods by working as practitioner at night with the army’s connivance (PARK, 2004: 436). In September 1957, when they were offered the opportunity to work for government agencies instead of the army, approximately 150 of them applied for 55 jobs.50) In February 1960, the situation did not improve, despite a discharge of 111 military doctors who served more than seven years.51) In 1961, the military doctors knew that they could be discharged by registering as candidates for an election, and approximately 200 officers, most of the 14 army hospitals, registered. The army was incapable of holding the veterans. In order to deal with the large-scale discharge movement that would endanger the army’s medical system, the government decided to recall 45 of those discharged through an election who did not complete their three-year term of service.52) In 1964, in response to the continuing decline in long-term service military doctors, the army extended the term of service for medical specialists to five years.53) However, even after that, there was no structural change suitable for the expanded scale, and the prospects of the army’s plan to maintain a huge evacuation system based on conscription and compulsion were not bright. Although the Korean army was able to expand the size of the medical evacuation chain rapidly in the wake of the war, the army’s medical system was fundamentally shaken both during and after the war.
6. Conclusion
As this article shows, Koreans who had no bases for military medical services rapidly developed the chain of medical evacuation in the wake of the Korean War. With the support of KMAG, the model of the Korean Army’s chain of medical evacuation was based on that of the US Army. Within a year of the outbreak of war, the Korean Army was able to build a nationwide evacuation chain from forward battalion aid stations to rear army hospitals. This application of a US-style medical system became a reference point for US military advisory group activities that would continue in Asia thereafter. One example was Taiwan, where a military advisory group was activated in 1951 and reorganized military medical system so that the Taiwanese military medical services were similar to those of the US military.54) The medical section of the Taiwan Advisory Group visited Korea during the Korean War and interacted with KMAG’s medical section.55)
However, the Korean Army’s expansion of medical evacuation chain during the Korean War resulted in instability. At the heart of the instability was manpower, rather than organization and transportation. In emergency situations, on-the-spot commissioned military doctors with no military bases accounted for more than 80% of the medical evacuation chain. The evacuations they conducted seemed to have operated successfully after 1951. However, the escalating war revealed the problems they faced. They did not sufficiently match up their actions with the aims of the army. Unlike the goal of the chain of medical evacuation, which attempted to prevent unnecessary evacuation in the front line and return as many mission-capable soldiers as possible in the rear to conserve fighting strength, on-the-spot commissioned doctors easily evacuated patients compared to the US Army in frontline and were reluctant to release patients to return to their duties in the rear hospitals. Korean Army doctors who were not sufficiently trained as military doctors struggled between the goals of military medical services and those of medical care. In this respect, the medical evacuations of the Korean Army during the Korean War demonstrates the fundamental tension between war and medicine.
Notes
George E. Armstrong, “Medical Service of the ROK Army”, RG 112, Entry UD-WW 96, Box 50, 1953. 2. 24, p. 4
For a study that explains the establishment of the US Military Advisory Group to the Republic of Korea (KMAG) in the context of US foreign military aid and the dispatch of Military Advisory Group, see PARK’s study (PARK, 2016).
For the initial period of military medical service, see (Yun, 1951; ROK Army Headquarters, 1959; SHIN, 1954)
“Historical Summation, Dept. of Public Health and Welfare, September 1945 – May 1947,” RG 332, Entry A1 1256, Box 40, pp. 8–9.
“Korean Army Medical School”, RG 319, Entry P 181, Box 3, 1950.
“Korean Army Medical School”, RG 319, Entry P 181, Box 3, 1950.
“Annex No. 10, Status of Training Supporting Arms and Services, K.A.,” Semi-Annual Report, Annexes 5-13, 1 Jan, 1950, RG 554, Entry A1 1355, Box 29, 1950, p. 6.
“Training of Korean Army Officers in Japan,” RG 319, Entry P 181, Box 3, 1950.
Oh Hyung Suck, “Individual Observer Report, 30 Day Prior,” RG 338, KMAG, Adjutant General, Decimal File, 1948-53, Box 30, 1950; Oh Hyung Suck, “Individual Observer Report, 30 Day Period,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 22, 1950; Hong Hwang Yong, “Individual Observer Report, 30 Day Period,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 22, 1950.
“Medical Department Data, Korean Army”, RG 319, Entry P 181, Box 3, 1950.
“Annex No. 10, Status of Training Supporting Arms and Services, K.A.,” pp. 4–7.
“Advisor’s Handbook,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 3, 1949, p. 37
“Annex No. I Present T/D and proposed reduction in KMAG Strength,” Semi-Annual Report, 1 Jan, 1950 – 30 June, 1950, RG 554, Entry A1 1355, 1950, Box 29.
Armstrong, “Medical Service of the ROK Army,” p. 2.
Surgeon General’s Office, Korean Army, “Annual Report of Medical Service Activities, Korean Army,” RG 112, Entry UD 1001, Box 199, 1951. 2. 22. p. 2.
Due to lack of people who could translate US military manuals, the important US field manuals such as FM 8-10 Medical Service, Theater of Operation, and FM 8-35 Transportation of Sick and Wounded were translated and issued in February 1952. Phillip J. Buckler (Lt Col, MSC, Senior Advisor), MFSS, ROKA, “Command Report for Medical Field Service School, Republic of Korea Army, 1 – 29 February 1952,” RG 407, Entry NM3 429, Non Organic Units, AYUT-8202 (8202nd Army Unit), US Military Advisory Group, Box 5787, 1952. 3. 15.
Surgeon General’s Office, Korean Army, “Annual Report of Medical Service Activities, Korean Army,” pp. 2-4.
“Report of Army Field Forces Observation Team No. 7 to FECOM(EXTRACT),” RG 112, Entry UD-WW 46, Box 69, 1952. 12, p. 1.
If there is no footnote on the evacuation process, see ROK Army’s FM 7-30 (ROK Army Headquarters, 1953).
“36 Yuggunbyeong-won-eseo wondaeboggwijanghaenghoe,” [A send-off party for returning soldiers in 36th Army Hospital] Chosun Ilbo, 14 November 1952.
Headquarters, Field Training Command, “Field Inspection of 7th ROK Division,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 40, 1951. 11. 17; “Inspection of Medical Company, 22nd Inf Regt, 1 Mile West of 3rd Div. C. P.,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 40, 1951. 12. 15; “Inspection of Medical Company, 18th Inf Regt, North Side of Han River near 3rd Div C. P.,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 40, 1951. 12. 14; “Inspection of Medical Co. 23rd Inf. Regt., 8 Miles West of 3rd Div. C. P.,” RG 338, KMAG, Adjutant General, Decimal File, 1948-53, Box 40, 1951. 12. 17.
John C. McKissick (Colonel, MC, Senior Medical Advisor) “Monthly Combat Operations Command Report (Reports Control Symbol CSGPO-28 (R1)),” RG 338, Entry A1 1361, Box 784, 1953. 6. 4.
“Medical Service and Evacuation Policies in Korea,” RG 112, Entry UD-WW 96, Box 50, 1951. 8. 8.
Harold P. Larson (Lt. Colonel, MSC), “Hospital Trains in Korea,” RG 112, Entry UD-WW 96, Box 50, 1951. 4. 16.
“Hyeondaejeon-ui jeongsu guggun,” [Armed Forces, The essence of modern warfare] Chosun Ilbo, 9 February 1953.
A. D. Sullivan (Lt. Colonel, MSC, Senior Advisor, MFSS) “Command Report for the Month of March,” RG 338, Entry A1 1361, Box 786, 1953. 4. 13.
Phillip J. Buckler, “An Introduction to the Medical Field Service School, Republic of Korea Army,” pp. 364–367.
KMAG, “Drafting of Medical Personnel, Republic of Korea,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 37, 1951.
“Report of Inspection of Army Medical School,” RG 338, KMAG, Adjutant General, Decimal File, 1948–53, Box 39, 1951. 5.
Arthur D. Sullivan (Lt Col, MSC, Senior Advisor), MFSS, ROKA, “Command Report for the Month of December, 1952,” RG 407, Entry NM3 429, Non Organic Units, AYUT-8202 (8202nd Army Unit), US Military Advisory Group, Box 5805, 1953. 1. 10, p. 21.
Senior Advisor, MFSS, ROKA, “History of MFSS, ROKA, for the month of January 1952,” RG 407, Entry NM3 429, Non Organic Units, AYUT-8202 (8202nd Army Unit), US Military Advisory Group, Box 5786, 1952. 3. 3.
Arthur D. Sullivan (Lt Col, MSC, Senior Advisor), MFSS, ROKA, “Command Report for the Month of January, 1953,” RG 407, Entry NM3 429, Box 5808, 1953. 2. 14; Arthur D. Sullivan, “Command Report for the Month of February, 1953,” RG 407, Entry NM3 429, Box 5810, 1953. 3. 17; Arthur D. Sullivan, “Command Report for the Month of March, 1953,” RG 407, Entry NM3 429, Box 5811, 1953. 4. 13; Arthur D. Sullivan, “Command Report for the Month of April, 1953,” RG 407, Entry NM3 429, Box 5813, 1953. 5. 12.
Since April 1953, the basic course had been extended to eight weeks, and approximately 200 students had been trained for eight weeks.
“Bogeonbu-wa tonghabmunje - jung,” [Ministry of Health and integration problems – second part] Kyunghyang Shinmun, 2 October 1953; “Mu-uichon-eun eonje eobs-eojina man myeong-e gae-eob-ui han salam,” [When will doctorless villages disappear? One practitioner for every 10,000 people] Dong-a Ilbo, 23 October 1953.
Some of the newly trained doctors were discharged immediately after completing their training (“Golyeonggun-uigwan-eul gyochehara,” [Replace the old military doctors] Chosun Ilbo, 6 March 1956).
For the north’s autumn offensive in 1952, see Institute for Military History, MND (Ministry of National Defense), 6.25 Jeonjangsa 10 [History of the Korean War 10] (Seoul, Korea: Institute for Military History, MND, 2012), pp. 330–331.
KMAG, “Command Report (November, 1952): Narrative Summary,” RG 407, Entry NM3 429, Non Organic Units, AYUT-8202 (8202nd Army Unit), US Military Advisory Group, Box, 5804, 1952. 11, p. 23.
John C. McKissick (Colonel, MC, Senior Medical Advisor), “Command Report,” RG 407, Entry NM3 429, Non Organic Units, AYUT-8202 (8202nd Army Unit), US Military Advisory Group, Box 5805, 1953. 12. 17.
John C. McKissick (Colonel, MC, Senior Medical Advisor), “Command Report,” RG 407, Entry NM3 429, Non Organic Units, AYUT-8202 (8202nd Army Unit), US Military Advisory Group, Box 5807, 1953. 1. 7.
During the Korean War, the shortage of military doctors was a chronic problem for the US military as well. Cowdrey, pp. 337–338.
KMAG, “Command Report (May, 1952): Narrative Summary,” RG 407, Entry NM3 429, Non Organic Units, AYUT-8202 (8202nd Army Unit), US Military Advisory Group, Box 5792, 1952. 5, p. 25.
For the war situation in 1953, see Institute for Military History, MND, 6.25 Jeonjangsa 11 [History of the Korean War 11] (Seoul, Korea: Institute for Military History, MND, 2013), pp. 177–178.
24 in original text. But considered an error.
McKissick, “Monthly Combat Operations Command Report (Reports Control Symbol CSGPO-28 (R1)),” 1953. 6. 4.
McKissick, “Monthly Combat Operations Command Report (Reports Control Symbol CSGPO-28 (R1)),” 1953. 6. 4.
“Gun-uigwan yebiyeog pyeon-ip gugbangjanggwan-e tan-won,” [The petition to Secretary of Defense for discharging military doctors], Dong-a Ilbo, 26 September 1955.
“Gun-uigwan-ui janggibogmu bulgapi,” [The military doctors’ Long-serving for the army is unavoidable] Chosun Ilbo, 13 March 1957.
“10 il-e jeon-yeog janggibogmu gun-uigwan,” [The long-term military doctors who will be discharged on the 10th] Chosun Ilbo, 1 July 1956; “31 il-e jeon-yeog” [Discharging on 31th] Chosun Ilbo, 30 May 1957.
“Bokmu-Yeonhan chogwa gun-uigwandeul jedae jinjung,” [The petition for discharge of military doctors who has exceeded the term of service] Dong-a Ilbo, 22 July 1956.
“5 nyeon isang bokmu 55 uimugwan jedae,” [The discharge of the 55 military doctors who served more than 5 years] Dong-a Ilbo, 27 September 1957; “Chong su 146 myeong,” [146 people in total] Chosun Ilbo, 9 October 1957.
“111 myeong yepyeon 7 nyeon isang doen gun-uigwan,” [111 military doctors with 7+ years of experience transferred to the reserve] Dong-a Ilbo, 12 February 1960.
“Hubang yuggunbyeong-won un-yeong-e keun jijang! 200 yeo myeong gun-uigwandeul jedae seodulleo,” [Disruptions to the rear army hospitals! Approximately 200 military doctors hurry to leave the army] Kyunghyang Shinmun, 12 March 1961; “Jeon-yeogdoen gun-uigwan dasi sojibkilo gag-ui uigyeol,” [The Cabinet decision to reconvene the military doctors who have been discharged] Kyunghyang Shinmun, 27 March 1961.
“Bokmy-yeonhan 5 nyeon-eulo yeonjang teuggi gun-uigwan,” [The medical specialists’ term of service extended to 5 years] Chosun Ilbo, 5 January 1964.
Formosa MAAG, “Resume of The Results of the Advisory Mission,” RG 112, Entry UD 1001, Box 223, 1953. 3.
Medical Advisory Section, “Daily Journal,” RG 338, Entry A1 1361, Box 784, 1953. 5.